Varicocele Embolization VS Microsurgery
When searching for the best varicocele surgeon in Delhi or evaluating varicocele treatment in Delhi, India, patients are often faced with a choice between traditional surgery and radiological procedures. In the specialized practice of Dr. Vijayant Govinda Gupta, a University Gold Medalist and world-record-holding urologist in New Delhi, we prioritize the “Gold Standard” approach to ensure your fertility and long-term health.
This comprehensive guide compares Microsurgical Subinguinal Varicocelectomy and Percutaneous Embolization, utilizing the latest 2025/2026 clinical data to help you make an informed decision for male infertility treatment in Delhi.
What is Microsurgery?
Microsurgical Subinguinal Varicocelectomy (MSV) is globally recognized as the most effective surgical treatment for varicoceles. It involves a microscopic-assisted ligation of the dilated veins through a tiny 2 cm incision in the groin.
Under a high-powered Zeiss Operating Microscope, Dr. Gupta performs a meticulous dissection that allows for:
Selective Ligation: Identifying and closing all abnormal veins (internal spermatic, cremasteric, and gubernacular) to ensure a near-zero recurrence rate.
Arterial Sparing: Using a micro-Doppler to preserve the testicular artery, preventing atrophy.
Lymphatic Preservation: Meticulously sparing delicate lymphatic channels to eliminate the risk of postoperative hydrocele (fluid buildup).
What is Embolization?
Percutaneous Varicocele Embolization is a non-surgical, minimally invasive procedure performed by an interventional radiologist. It is often marketed as a “no-incision” alternative, though it relies on different clinical mechanisms.
Using Continuous Fluoroscopy (Live X-rays), the radiologist inserts a catheter through a vein in the groin or neck and uses metallic coils or liquid sclerosants to block the blood flow. While it avoids a surgical incision, it cannot address accessory veins located outside the main spermatic cord, which can lead to higher recurrence rates in complex cases.
Difference between Microsurgery and Embolization
| Parameter | Microsurgical Varicocelectomy (MSV) | Varicocele Embolization (Percutaneous) |
| Success Rate | 99% (Gold Standard) | 80–90% |
| Recurrence Rate | Less than 1% (SUCRA: 91.6%) | 10–20% |
| Radiation Exposure | $0$ mSv (None) | $18$ mSv (Significant) |
| Fertility Impact | Highest Motility Rank (82.9%) | Lower Motility Rank (58.7%) |
| Hydrocele Risk | Near Zero (with Lymphatic Sparing) | Minimal |
| Recovery Time | 2–3 Days (Return to work) | 1–2 Days (Return to work) |
| Bilateral Repair | Highly Reliable | 19.3% Technical Failure on Right |
Scientific References & Citations
Surgical approaches to varicocele: a systematic review and network meta-analysis.
Source: Asian Journal of Andrology (2025).
DOI: 10.4103/aja202541.
Key Finding: This is the source for the SUCRA rankings, which prove that Microsurgery (MSV) is Ranked #1 for preventing recurrence (91.6%) and improving sperm motility (82.9%).
Impact of varicocele repair on semen parameters and spontaneous pregnancy.
Source: Arab Journal of Urology (2024).
Key Finding: Confirms that microsurgical repair leads to the highest probability of spontaneous pregnancy compared to other methods.
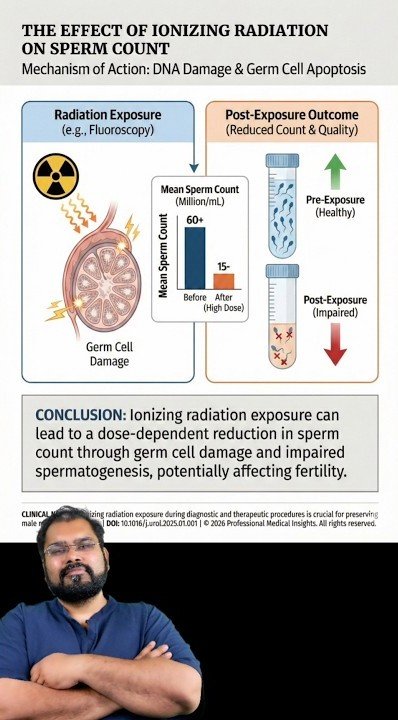
Heller, C. G., et al. Effects of ionizing radiation on the human testis.
Source: Radiobiology Consensus Data.
Key Finding: Established that the human testis is extremely sensitive to radiation; doses as low as 15 rads can stop sperm production.
Rowley, M. J., et al. Effect of graded doses of ionizing radiation on the human testis.
Key Finding: Provides long-term data on how radiation exposure (like that used in Embolization) can lead to extended suppression of sperm count.
Linear No-Threshold (LNT) Model of Radiation Risk.
Source: Committee on the Biological Effects of Ionizing Radiation (BEIR).
Key Finding: The scientific gold standard states there is no safe dose of radiation for germ cells (sperm DNA).
Videos On Embolization
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
What is Superior? Varicocele Microsurgery VS Embolization
For patients seeking the best varicocele treatment in India, the landmark 2025 Network Meta-Analysis (NMA) by Lin-Jie Lu et al. provides a definitive answer based on SUCRA (Surface Under the Cumulative Ranking Curve) scores.
1. Best for Recurrence Prevention
The Lin-Jie Lu study ranks MSV as #1 for reducing postoperative recurrence, with a SUCRA score of 91.6%. Embolization and traditional open surgery rank significantly lower, making microsurgery the preferred choice for a permanent cure.
2. Best for Sperm Motility Improvement
Data highlights that Microsurgery (MIV/MSV) is the most effective intervention for increasing sperm motility, achieving an 82.9% rank. In contrast, embolization ranks at 58.7%, meaning microsurgery offers a statistically better chance of improving natural conception rates.
3. The "No Safe Dose" Radiation Reality
A critical safety difference is the exposure to ionizing radiation.
Embolization: Patients are exposed to a mean effective dose of $18$ mSv—equivalent to approximately 900 chest X-rays focused on the pelvis.
Microsurgery:This procedure is 100% radiation-free ($0$ mSv). According to the Linear No-Threshold (LNT) model, there is no safe dose of radiation for the gonads. Ionizing radiation can cause Germ Cell Damage and Sperm DNA Fragmentation (SDF), which is counterproductive for men seeking to improve their fertility.
Varicocele Surgery Cost in Delhi, India
Transparency in pricing is a hallmark of Dr. Vijayant Govinda Gupta’s practice. As of 2025/2026, the cost of microscopic varicocele surgery in Delhi is:
Unilateral (One Side): Approximately ₹40,000 ($1,000 for international patients).
Bilateral (Both Sides): Approximately ₹50,000 ($1,200 for international patients).
This pricing is often more affordable than the varicocele embolization cost in India, which can range from ₹1,25,000 to ₹1,60,000 due to the high cost of interventional equipment and coil materials.
FAQs on Varicocele Microsurgery and Embolization
For patients seeking the best varicocele treatment in India, the landmark 2025 Network Meta-Analysis (NMA) by Lin-Jie Lu et al. provides a definitive answer based on SUCRA (Surface Under the Cumulative Ranking Curve) scores.
Microsurgical varicocelectomy is a precise surgical procedure performed by a urologist using a high-powered microscope to ligate veins, whereas embolization is a non-surgical radiological procedure performed by an interventional radiologist who blocks veins from the inside using coils or liquid agents.
It is categorized as the gold standard because it offers the highest success rates (over 99%), the lowest recurrence rates (less than 1%), and effectively preserves the testicular artery and lymphatics to prevent complications.
Yes, it is considered a minimally invasive interventional radiological procedure. It involves only a tiny needle stick in the groin or neck to access the venous system and does not require a surgical incision.
According to the latest 2025/2026 meta-analysis by Lin-Jie Lu et al., microsurgical approaches (MIV/MSV) have the highest effectiveness in increasing sperm motility, with a ranking of 82.9% compared to 58.7% for coil embolization.
Microsurgery has a recurrence rate of less than 1%, while embolization has a significantly higher recurrence risk, typically ranging from 10% to 20% depending on the patient's anatomy.
Yes. Technical failure occurs in about 19% of right-sided or bilateral embolization attempts because the right spermatic vein enters the body at a difficult angle that a catheter may not be able to navigate.
Yes. Both treatments can improve semen quality, but microsurgery is statistically more effective in reducing Sperm DNA Fragmentation (SDF), which increases the chances of both natural pregnancy and successful IVF outcomes.
No. Microsurgery is a purely mechanical procedure and involves 0 mSv of radiation exposure.
Embolization uses fluoroscopy (live X-rays), which results in a mean effective radiation dose of approximately 18 mSv. This is roughly equivalent to 900 chest X-rays focused on the pelvic region.
In microsurgery, the risk is extremely low (0.7% to 2.1%) because the microscope allows the surgeon to see and spare the lymphatic vessels. Embolization also has a very low risk of hydrocele because it does not involve external dissection of the spermatic cord.
Embolization recovery is very fast, with most patients returning to normal activities within 24 to 48 hours. Microsurgery recovery is slightly longer but still rapid; patients are typically back to sedentary work within 2 to 3 days and full activity in 1 to 2 weeks.